









Work Standard and Standard Work

It has taken me a while to understand the distinction and implications between these two sets of words. Does the order of these two words really matter? Yes!
A work standard is a definition that tells a production system the aim. Standard work is the process by which the production system tries to apply the work standard. To clarify the process nature of standard work, some people like to use the term standardized work. Perhaps we should use the phrase ‘standardizing work’ to really drive home this point!
Example
In one of my projects, ICU teams are working to reduce ventilated-acquired pneumonia (VAP). From the patient’s perspective, the ICU should care for each patient in a way that no patient suffers VAP. The ICUs need a clear definition of VAP to track performance relative to this aim.
The ICU teams have accepted a bundle of actions and protocols. One of the actions includes a condition to have beds elevated 30⁰.
The nurses and support staff need a simple way to determine whether beds are correctly elevated. If beds are not elevated correctly for every patient every day, then the team needs to come up with one or more changes. What could be done to make it easy to see if each bed is elevated correctly?
Work Standard
In practice, a work standard is a current best representation, subject to revision. Logically, a work standard precedes standard work.
Isao Kato describes the Toyota approach to standard work in five step-ups.
Work standards comprise step-up 1. Work standards should be the operational definition of product or service the customer will receive. If the work standards are met, the customer will get the intended product or service.
Kato helpfully distinguishes three elements of a work standard:
(1) An output work standard. This standard defines the product or service. In old-fashioned acceptance sampling terms, the output work standard defines whether we declare the product or service acceptable or not. In the ICU, we want each patient free from VAP.
(2) An equipment and environmental conditions work standard. This standard defines the settings and levels of equipment and environmental conditions the producer requires to achieve the output. The elevation of bed to 30⁰ is an example.
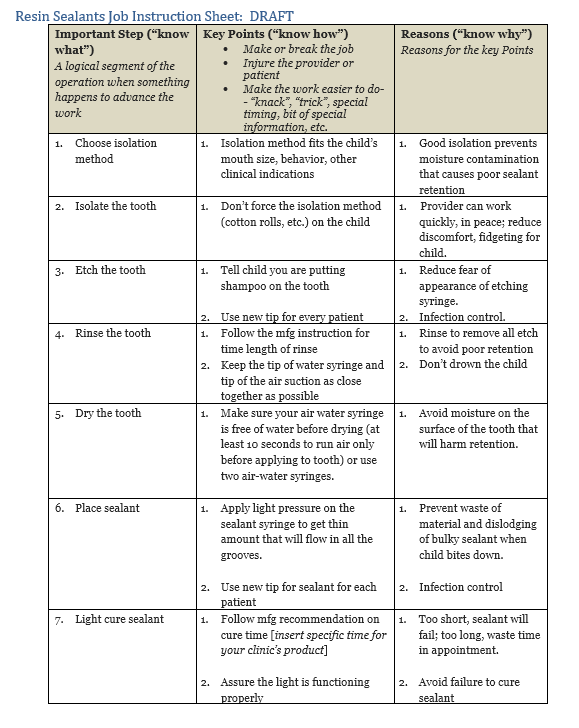
(3) An operation/person work standard. This standard defines the work tasks in sequence that will yield the agreed-to product or service, interacting with equipment and environment. Who should assure that each bed is at 30⁰?
Work standard (1) translates what the customer wants into production language. Work standards (2) and (3) complete the definition. Kato uses the word ‘Normal’ to describe the desired product or service, in the sense of a norm. Normal is what the producer aims to achieve. Abnormal is what often gets produced instead.
Work standards (1), (2), and (3) define how to produce the desired outcome, as sketched in the Step-up 1 Causal Theory picture.
Standard Work
Using Kato’s outline, Step-ups 2 and 3 are the core of the standard work process.
Step-up 2 directs us to make it easy to see departures from normal. Kato says: “Make it easy to see abnormal.”
Can you easily see whether the product or service produced matches the output standard?
Can you easily see whether the equipment and environmental conditions match the equipment and environmental standard?
Can you easily see whether the operations match the operation/person work standard?
Step-up 2 aims to eliminate the need for expert judgment and detailed study, which usually mean delays and wasted effort.
In some ICUs the wall in each room is marked with tape to show the correct elevation to prevent VAP. Anyone can see quickly whether the bed elevation matches the mark or not.
Step-up 3 recognizes that actual production inevitably will vary from the aim defined by the work standard. If it is easy to see whether beds are elevated to 30⁰, then it is simple to audit the current conditions relative to the standard.
The gap between the aim and actual production is the essence of an operations problem. If three out of 12 beds are not elevated to 30⁰, what can you do to come up with a change to reduce or eliminate the three-bed problem? Direct observation and then reflection about potential causes and solutions will drive your creativity. The daily problems pull you to practice PDSA rather than PDSA reserved for special, occasional applications.
The activities in Step-ups 2 and 3 are linked and mutually reinforcing. I can imagine that a solution to a problem may lead to changes to the work standard. For example, if there is a problem with bed elevation in the ICU, detective work and PDSA testing might lead to edits to the operation/person work standard. I need to study how the ICU teams tackle their work standard and standard work to understand this point further.
A note about training
Training fits into Step-up 2 because training helps people distinguish normal from abnormal.
The secret of training: focus training on aspects of work that people “Don’t know” or “Can’t do”.
A key insight from Oscar Roche and his colleagues: delay extensive training until you have worked on making it easy to see abnormal output, settings and operations. Your training will be simpler and easier to grasp because ‘easy to see’ work will reduce ‘Don’t know’ and ‘Can’t do’ to more manageable levels.